⚕ Clinician Reference
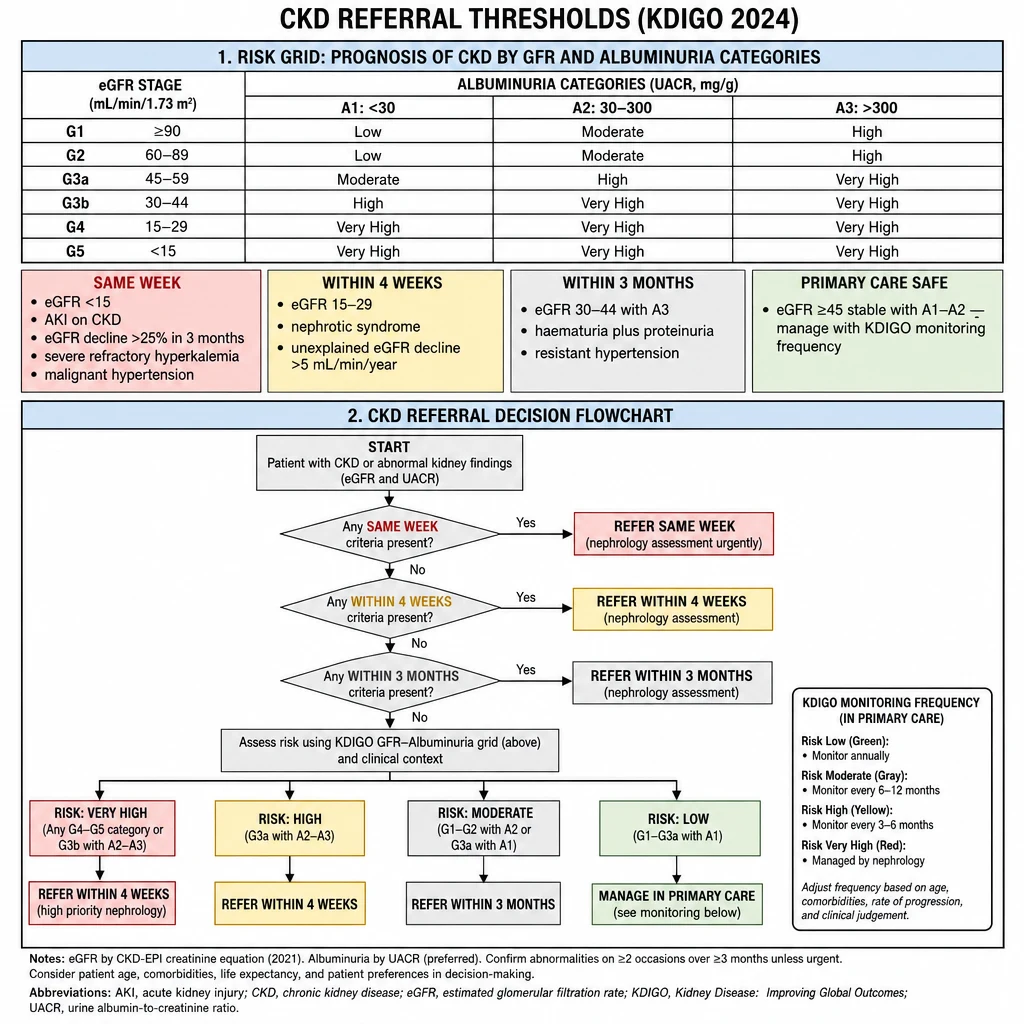
KDIGO (Kidney Disease: Improving Global Outcomes) 2024
🇵🇭 Philippines Context
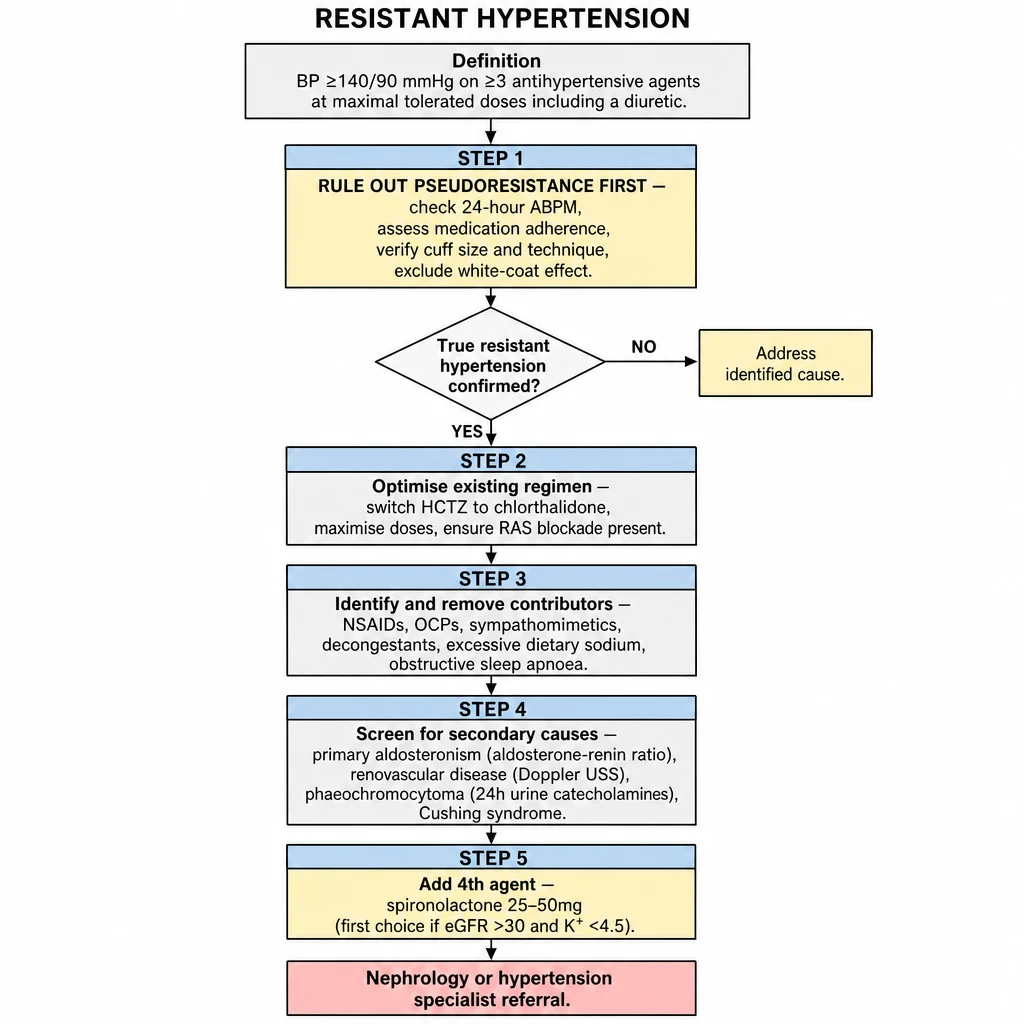
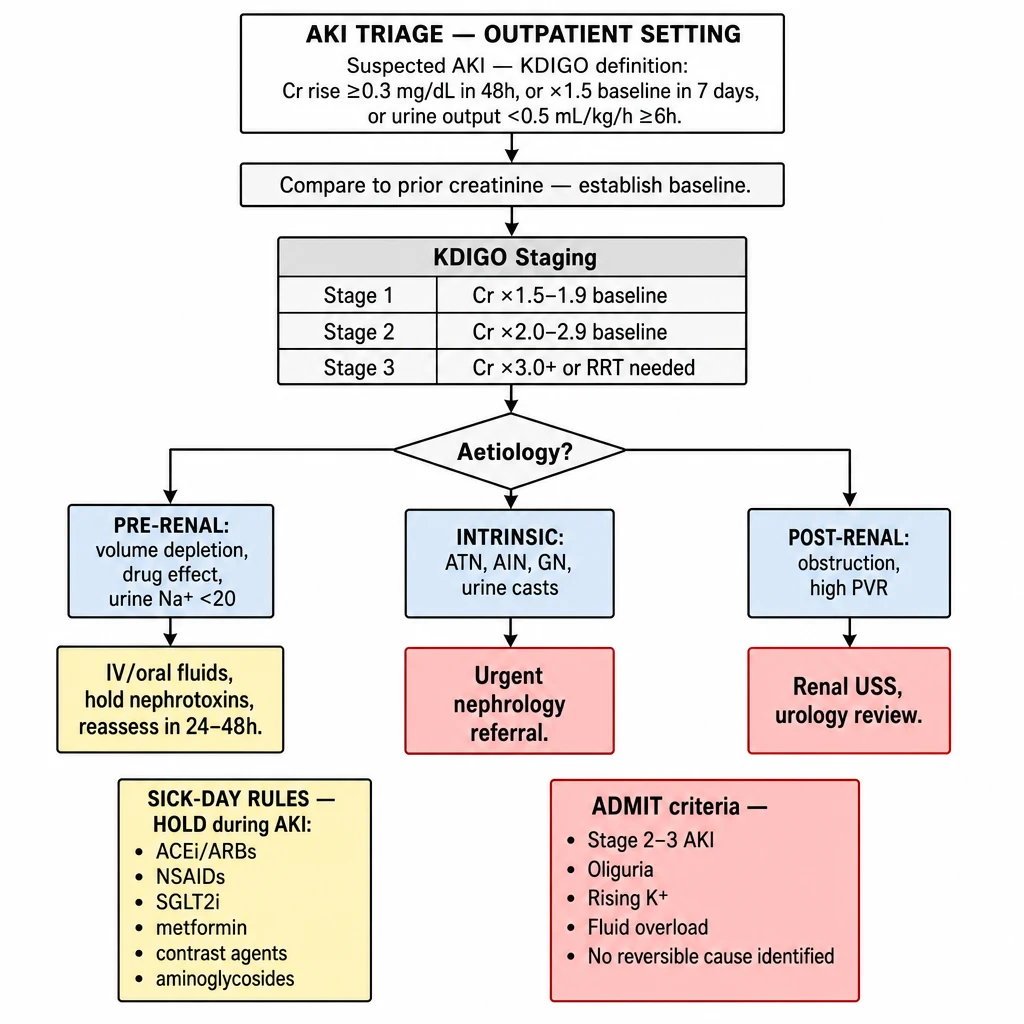
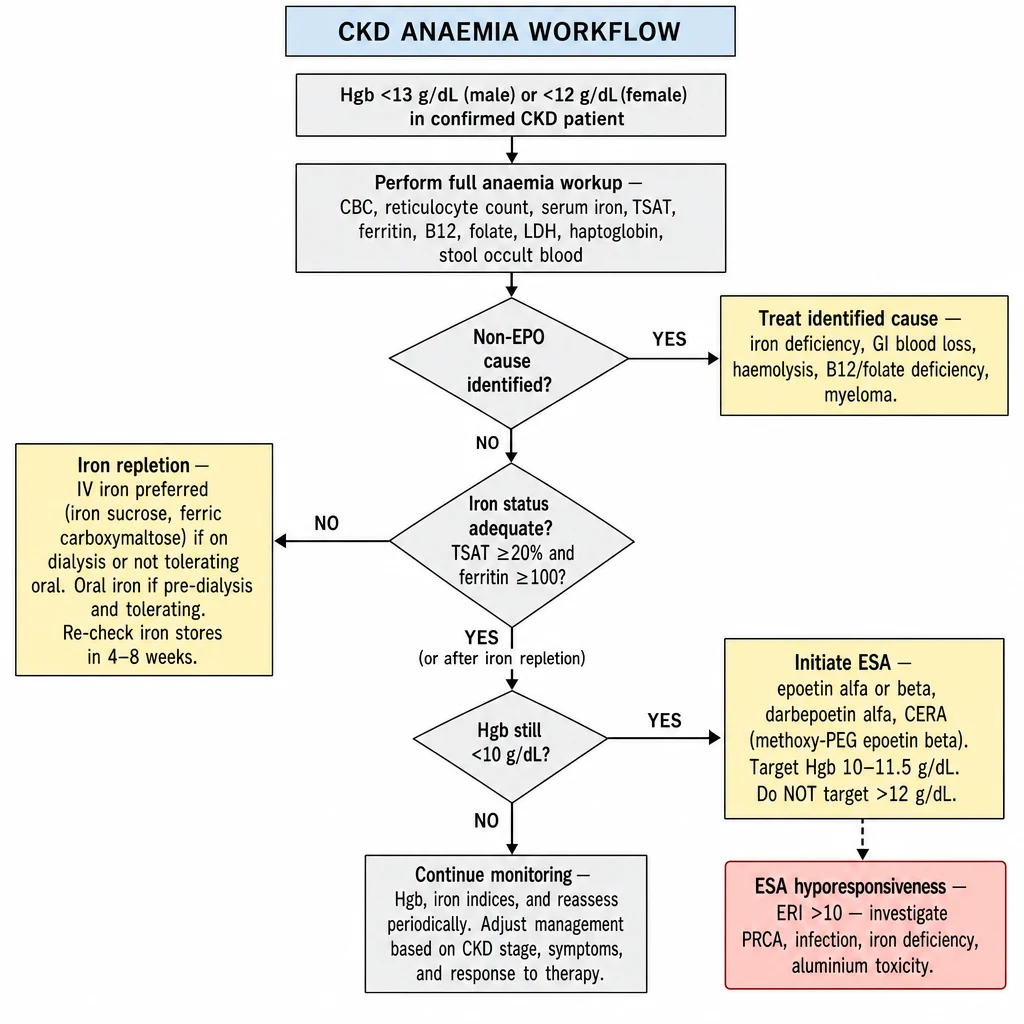
Practical Outpatient Algorithms
9 rapid decision pathways for nephrology & general medicine
Designed for GPs and IM residents managing common renal and metabolic problems in the outpatient setting. Each algorithm distills current KDIGO, ACC/AHA, and local DOH guidance into actionable decision steps.